Neuronal intranuclear inclusion disease (NIID)
We are now carrying out clinical research, genetical research and pathological research of neuronal intranuclear inclusion disease (NIID) at Suzuka National Hospital.
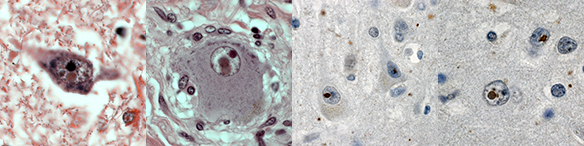
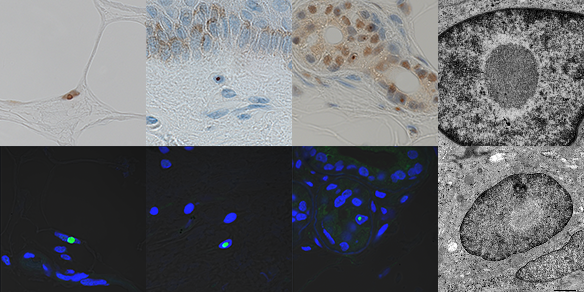
NIID is a neurodegenerative disease whose main symptoms are forgetfulness (dementia) and muscular weakness of the limbs, and /or ataxia. The first case of NIID was reported in 1968, and since then NIID cases has been diagnosed and reported with same histopathological features of ubiquitin-positive intranuclear inclusion from autopsy samples (Figure 1). In 2011, we discovered and reported that skin biopsy is useful for the diagnosis of NIID (Figure 2), afterwards the number of NIID case reports has dramatically increased.
- Figure 1: NIID histological findings
- Figure 2: NIID skin biopsy findings
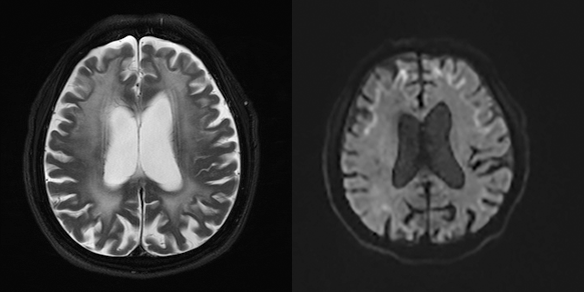
In particular, many cases were diagnosed as NIID that initial symptom was forgetfulness occurs in the elderly, and showing abnormal white matter high intensity signals in head MRI T2 imaging and abnormal high intensity signals along the corticomedullary junction in diffusion weighted imaging (DWI) (Figure 3). Such MRI T2 findings look very much alike the MRI finding of chronic ischemic change, many NIID cases may have been overlooked till now.
- Figure 3: Head MRI findings for NIID
Suzuka National Hospital is the unique institute that has plenty of experience of NIID diagnosis by skin biopsy samples.
Please contact us if you find a suspected case of NIID.
We are now studying many cases of NIID at Suzuka National Hospital, and promoting clinical research of NIID and genetical research, especially the relationship of clinical symptoms between genetical repeat expansion, and developing radial remedy of NIID (e-mail: niiddiagnosis@gmail.com).
Literature References
- Sone J, Mitsuhashi S, Fujita A et al. Long-read sequencing identifies GGC repeat expansions in NOTCH2NLC associated with neuronal intranuclear inclusion disease. Nature Genetics, 51:1213-1221, 2019.
- Lindenberg R, Rubinstein LJ, Herman MM et al. A light and electron microscopy study of an unusual widespread nuclear inclusion body disease. A possible residuum of an old herpesvirus infection. Acta Neuropathol (Berl) , 10(1):54-73.1968.
- Takahashi-Fujigasaki J: Neuronal intranuclear hyaline inclusion disease. Neuropathology, 23(4):351-359. 2003.
- Sone J, Mori K, Inagaki T et al. Clinicopathological features of adult-onset neuronal intranuclear inclusion disease.
Brain;139(12):3170-3186, 2016. - Sone J, Kitagawa N, Sugawara E et al.: Neuronal intranuclear inclusion disease cases with leukoencephalopathy diagnosed via skin biopsy. J Neurol Neurosurg Psychiatry; 85(3): 354-6, 2014.
- Sone J, Tanaka F, Koike H et al. :Skin biopsy is useful for the antemortem diagnosis of neuronal intranuclear inclusion disease. Neurology 76(16): 1372-1376, 2011.
- Sone J, Hishikawa N, Koike H et al. :Neuronal intranuclear hyaline inclusion disease showing motor-sensory and autonomic neuropathy. Neurology;65(10):1538-1543, 2005.